
Safeguarding
Vulnerable Adults
Introduction
This policy sets out the roles and responsibilities of DDCS in working together with other professionals and agencies in promoting adults’ welfare and safeguarding them from abuse and neglect. DDCS believes that the welfare of adults is paramount and that an adult has a right to feel safe and protected from any situation or practice that results in them being harmed or at risk of harm. DDCS is committed to maximising people’s choice, control and inclusion and protecting their human rights as important ways of meeting their individual needs and reducing the potential for abuse.
A note on Equality and Diversity
This policy has been developed in line with DDCS’ principles of Equality and Diversity and is underpinned by the following standards:
■ An adult’s welfare and safety is everyone’s responsibility.
■ Staff must work together, understand and appreciate other professionals’ roles and responsibilities.
■ No one must be discriminated against on the grounds of age, race, ethnicity, religion, culture, class, sexual orientation, gender or disability.
The Care Quality Commission’s (CQC) “Essential Standards of Quality and Safety” states that all people who use services from a health organisation should be protected from abuse, or the risk of abuse, and their human rights be respected and upheld.
The first priority should always be to ensure the safety and protection of vulnerable adults. It is the responsibility of all staff to act on any suspicion or evidence of abuse or neglect and to pass on their concerns to a responsible person/agency (Public Interest Disclosure Act 1998).
All those making a complaint or allegation or expressing concern, whether they be staff, Service Users, carers, or members of the general public, should be reassured that:
■ They will be taken seriously.
■ Their comments will usually be treated confidentially but their concerns may be shared if they or others are at significant risk.
■ Service Users will be given immediate protection from the risk of reprisals or intimidation.
■ If staff, they will be given support and afforded protection, if necessary, e.g.: under the Public Interest Disclosure Act 1998 they will be dealt with in a fair and equitable manner; and
■ They will be kept informed of any action taken and the outcome.
The safeguarding and promotion of the welfare of vulnerable adults is an integral element of the services and care offered by all staff in both statutory and voluntary and community sector organisations working on behalf of Dan Devitt Consultancy Services (DDCS).
The service offer delivered via or on behalf of DDCS is potentially very broad in nature and could therefore include care offered to children, young people, families or adults who are parents or carers, and potentially require both awareness and both adults and children’s safeguarding approaches.
The aim of the policy is to ensure that there is a robust system in place to safeguard Vulnerable Adults who receive service from DDCS and to support staff with safeguarding Vulnerable Adults. The policy sets out the roles and responsibilities of all staff and those working on behalf of DDCS with respect to keeping Vulnerable Adults and promoting their welfare.
-
Dan Devitt Consultancy Services do not currently or foreseeably have any direct contracted or subcontracted relationship or operate on its own as either a provider of services to the community where direct care or clinical provision to Vulnerable Adults would be conducted by DDCS itself.
That limitation on the scope of activities delivered by DDCS notwithstanding this policy has been drafted to ensure that DDCS is well placed to ensure that it is delivering a comprehensive approach to Safeguarding (both Vulnerable Adults and CYP) and related policies and able to adapt to future changes in commissioned activities. It stands as a visible sign of DDCS’ awareness of and commitment to the provision of safeguarding and related assurance for services that are delivered through DDCS via subcontracted entities and with a view to ensuring compliance is built into the DDCS policy framework before rather than after it becomes necessary.
DDCS’ work varies in scope across counties and local NHS Trusts, creating relationships between DDCS and Local authorities, NHS, public health providers, and other relevant organisations.
These organisations do not currently perform functions where adults safeguarding (or children’s) functions are entailed, but this is a situation that could potentially change over time.
To provide assurance of DDCS’ robust and forward-thinking approach to safeguarding this policy and others on different safeguarding themes have been drafted in preparation in case any of the functions do, one day, become an element of DDCS business.
DDCS will ensure that it monitors and provides assurance to its commissioners that its relationships – either to commissioning bodies or subcontracted entities - align with its commitment and obligations and accountability to commissioners for safeguarding practice and policies in subcontractors.
This will be reviewed on a regular and ongoing basis and especially at the commencement of new contractual relationships where an assessment to ensure a full compliance with relevant safeguarding practice and policies is conducted.
In this way DDCS will evolve its safeguarding response in line with future requirements whilst constantly assessing, reflecting upon and improving its safeguarding approach and policy suite.
-
The Policy is intended to support all DDCS staff and subcontractors working on behalf of DDCS with safeguarding adults within all geographical areas in which services are delivered.
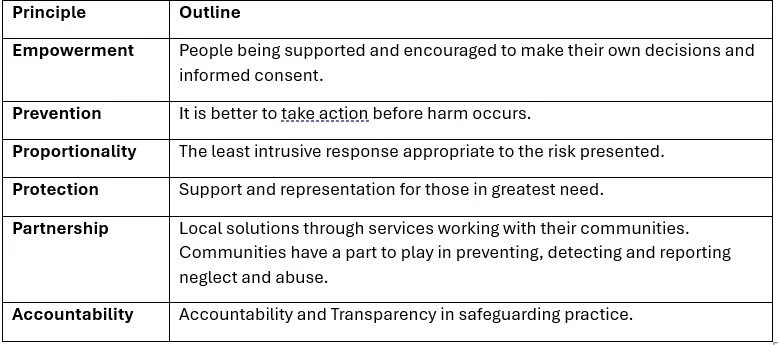
DDCS’ Vulnerable Adult Safeguarding Policy, procedures and responsibilities are guided by the 6 principles of Care Act 2014 shown below in Table 1.
This Policy also informs all staff within Provide of statutory responsibilities and expected practice regarding issues related to Honour Based Abuse (HBA), Forced Marriage and Female Genital Mutilation (FGM).
The Care Act 2014 established a new statutory framework for care and support, including adult safeguarding.
Safeguarding adults is integral to complying with local and national legislation/regulations. This is achieved close adherence and multi-agency working via local Adults Safeguarding Boards.
Currently the majority of DDCS works will fall within different regions’ operational contexts, despite the company’s base in London. It is intended that this policy and those covering other key safeguarding agendas will provide a robust and comprehensive policy approach to underpin operations in other areas or regions and meet the needs of other relevant Adult Safeguarding Boards.
The Intercollegiate Document ‘https://www.rcn.org.uk/Professional-Development/publications/adult-safeguarding-roles-and-competencies-for-health-care-staff-uk-pub-007-069, sets out the levels of competencies expected of all staff working within the health service with regards to adults safeguarding.
All staff must ensure that they possess the required knowledge, skills and competencies – in line with their role as set out in their training matrix in line with the Intercollegiate Document (2019).
See Care Act 2014 (legislation.gov.uk) and Care Act factsheets - GOV.UK (www.gov.uk)
-
The purpose of this policy is to ensure that DDCS Staff and subcontracted entities are able to appropriately fulfil their safeguarding obligations with regards to Vulnerable Adults.
DDCS accepts the principles laid down within the Local Safeguarding Adults Board Guidelines and is committed to:
■ Take action to identify and prevent abuse from happening.
■ Respond appropriately when abuse has or is suspected to have occurred.
■ Ensure that the agreed safeguarding procedures are always followed.
■ Offer/deliver support, advice and resources to staff in responding to safeguarding issues.
■ Inform staff of any local or national issues relating to safeguarding adults.
■ Ensure staff are aware of their responsibilities to attend training and to support staff in accessing these events.
■ Ensure that the organisation has a dedicated staff member with an expertise in safeguarding adults.
■ Ensure staff have access to appropriate consultation and supervision regarding safeguarding adults.
■ Understand how diversity, beliefs and values of people who use services may influence the identification, prevention and response to safeguarding concerns.
■ Ensure that information is available for people that use services & family members setting out what to do if they have a concern (e.g. ASK SAL helpline).
■ Complies with several safety and identity checks on appropriate by Disclosure Barring Service (DBS 2014).
■ Job descriptions for staff that contain a statement regarding staff responsibility for safeguarding children and adults.
All staff must be aware of and understand the risk factors for abuse and what they must do if a person is being abused, suspected of being abused, is at risk of abuse or has been abused.
DDCS will work collaboratively with other services, teams, individuals and agencies in relation to all safeguarding matters and has safeguarding policies that link with Local Authority policies. It participates in the LSAB where required; has clear procedures which are followed in practice, monitored and reviewed in the context of safeguarding and considers relevant guidance set out in the CQC’s schedule of applicable publications.
DDCS understands that the safety, rights and wellbeing of service users is paramount and that they have a right to feel safe and protected from any situation or practice that results in them being harmed or at risk of harm. DDCS is committed to ensuring the primacy of service users human rights, choice; and their right to control and be included in care/decision making.
DDCS understands these are important for meeting the individual needs of service users and reducing the potential for abuse. It is therefore central to the DDCS Safeguarding response.
-
The policy applies to all staff employed or working on behalf of DDCS. This includes those that are:
■ Full or Part Time directly employed Staff
■ Executive Leadership staff supporting DDCS
■ Temporary, voluntary, contracted or self-employed staff
■ Consultants and agency staff
The above will be referred to as ‘all staff’ in the policy.
-
All staff
All staff must always be alert to the possibility of significant harm to adults through abuse or neglect, or to an adult who is at-risk. All staff should be able to recognise indicators and know how to act upon concerns, their depth of knowledge being commensurate with their roles and responsibilities.
Effective safeguarding arrangements should aim to meet the following two key principles:
■ Safeguarding is everyone's responsibility: for services to be effective each individual and organisation should play their full part; and
■ A person- centred approach: for services to be effective they should be based on a clear understanding of the needs and views of vulnerable adults.
All staff must be aware of:
■ the vulnerabilities of certain groups of people such as those who are disabled, ‘looked after’, and socially excluded.
■ the vulnerabilities of certain groups of adults who may find parenting difficult.
The latter category can include a very wide range of people and touch upon a broad range of conditions, and agendas. For example, those experiencing domestic abuse coercive control and or violence, instability arising from complexity involving mental health conditions or problems, uncontrolled substance or alcohol misuse, learning disabilities, involvement with the justice system or exposure to the effects of criminality, violence and the drugs trade, or those with unmet support needs and those exposed to economic adversity, poverty and stresses arising from the cost-of-living crisis.
Core Principles
All staff must therefore be aware of relevant adult safeguarding policies and procedures which may be involved including where incidents of children and young people potentially abusing vulnerable parents or carers.
All staff working primarily with adults who are parents or carers should always consider the effects on parenting capacity and subsequent implications for children of the adult’s illness or behaviour.
All staff must recognise that sharing information is vital for early intervention to ensure that adults are protected from abuse and neglect and that safeguarding is paramount and can override any duty of confidentiality.
All staff regardless of grade or position must follow local SAB Procedures where there are concerns that a child is being abused or when there are adult safeguarding concerns. This cannot be delegated to others.
All staff should be aware that when they have concerns about possible adult abuse or neglect, they can discuss their concerns with the DDCS Safeguarding Lead or a Local Safeguarding Adults Board advisor or local NHS Named/Designated Safeguarding Professional, Manager or Supervisor, as required and must know how to access this support.
IN EMERGENCIES
If emergency action is needed to protect an adult this should never be delayed due to the need to discuss concerns.
See below for the process for actioning immediate concerns as referenced in the NHS guidance: Abuse and neglect of Adults at risk.
Key contacts and numbers to discuss an adult’s safeguarding issue:
■ If a person is in immediate danger, call 999.
■ If you're worried that an adult is being abused, contact the adult social care team at their local council. You can use this NHS search tool to find Local Adult Social Care contacts.
■ If you’re worried that an older person is being abused, you can also call the 24/7 confidential Hourglass helpline at 0808 808 8141.
All staff should uphold the rights of the adult to be able to communicate, be heard and safeguarded from harm and exploitation whatever their race, religion, language, ethnicity, gender, sexuality, age, health or disability, location/placement, criminal behaviour, political or immigration status.
Those who work directly with children/young people should also have access to the Local SCB Child Protection procedures. (See Safeguarding Adults Executive Board – London Multi-Agency Adult Safeguarding Policy & Procedures). LSAB Procedures may be available electronically. If staff print or save copies, they are responsible for ensuring these remain updated.
All staff must undertake mandatory adult, child and young person safeguarding training at a level that is appropriate for their role and commensurate with the operational requirements of their post, and reflects the competencies within the Intercollegiate Guidelines as set out in Safeguarding Children and Young People: Roles and Competencies for Healthcare Staff (RCN 2019).
All staff must ensure that they update their skills and knowledge by undertaking further refresher training as appropriate and in line with level of competency.
Assurance of this compliance will be through an annual audit process delivered by the DDCS Safeguarding Lead and assured by the DDCS Director. This will be refreshed in line with contractual obligations rather than strictly by calendar year to ensure that assurance is quickly developed for new areas of operation or focus, rather than waiting on a calendar bound process.
All staff that work regularly with adults are responsible for ensuring that they access ongoing safeguarding adults supervision depending on the recommendations for the practice area.
DDCS Director
The DDCS Chair has overall responsibility for ensuring that the DDCS contribution for safeguarding and promoting the welfare of vulnerable adults and children is discharged effectively for all adults, children & young people for whom Providers or partnerships deliver services. This includes ensuring that:
■ there are safe and robust operational arrangements in place for safeguarding adults and children in all the services that are provided.
■ staff work in line with Local Safeguarding Adults Procedures, and any other locally agreed policies and guidance.
Operational responsibility for maintenance and updates to the policy are delegated by the Director to the DDCS Safeguarding Lead and the Safeguarding Lead’s performance is assured by the Director.
DDCS Safeguarding Lead
The DDCS Safeguarding Lead provides professional leadership and strategic direction on DDCS safeguarding adults related activities or services to provide a coordinated and integrated safeguarding service that evolves in time with DDCS.
It is the responsibility of the DDCS Safeguarding Lead to ensure that contracted services are delivered in accordance with the Safeguarding Adults Policy and Guidelines and that there are safe systems and processes in place to support DDCS contracted services.
The DDCS Safeguarding Lead is responsible for ensuring that the needs of all adults, children and young people are at the forefront of DDCS delivery planning and contractual negotiations and that high quality health services that meet identified quality standards are delivered.
The DDCS Safeguarding Lead will ensure that monitoring and reporting of safeguarding activity to fulfil the relevant and appropriate requirements under CQC Essential Standard of quality and safety (2010), Local Safeguarding Guidance and recommendations from Serious Case Reviews takes place.
The DDCS Safeguarding Lead is responsible for promoting good professional practice and providing specialist advice and support to DDCS staff and subcontractors on any issue relating to safeguarding adults.
The DDCS Safeguarding Lead will ensure provision of safeguarding adult supervision and training to staff, regular audits of practice and conduct the internal Management Reviews (IMR’s) as part of Serious Case Reviews or under a regular audit or to investigate an incident.
The DDCS Safeguarding Lead will ensure that DDCS is represented at the health subgroup of Local Safeguarding Adults Boards (LSCBs) if necessary.
All DDCS Staff are required to ensure that:
■ agreed safeguarding adults procedures are always followed and to become familiar with any issues relating to adult safeguarding through participation in safeguarding training and to maintain current knowledge and skill.
■ all safeguarding concerns are discussed with the adult safeguarding lead and that decision in relation to the handling of these concerns are recorded.
■ appropriate forms are completed to raise a safeguarding concern based on each LSABs requirements and submitted without any avoidable delay and copies of all forms are sent to the DDCS Safeguarding Lead.
■ health professionals leading on adult safeguarding enquiries do so within set timescales agreed with the LSAB and other multi agencies.
■ Staff attend relevant adult safeguarding training at a level appropriate to role and responsibility, and to ensure staff identify their training needs regarding safeguarding adults and access appropriate training and this process is formalised through management supervision and appraisal processes.
Additional Responsibilities of all DDCS Staff
■ To know the location and the contents of the LSAB and DDCS Safeguarding Vulnerable Adults Policies and Guidance.
■ Participate in safeguarding adults training relevant to post and professional responsibilities and maintain current working knowledge.
■ Refer to and adhere to the safeguarding policies and procedures at all times, particularly if concerns arise about the safety or welfare of an adult with care and support needs.
■ Discuss any concerns about the welfare of an adult with care and support needs with the Line Manager and the DDCS Safeguarding Lead.
■ Contribute to actions required including information sharing and attending meetings relating to the safeguarding adults.
■ Work collaboratively with other agencies to safeguard and protect the welfare of people who use DDCS contracted services.
■ Always remain alert to the possibility of abuse.
■ Recognise the impact that diversity, beliefs and values of people who use services can have.
-
DDCS exists (as set out in section 1. above) to provide a vehicle for commissioned services and contracting arrangements that cannot be easily fulfilled by the constitutional structure of organisational environment in a particular circumstance. As a result of this, DDCS is involved explicitly in the contracting and commissioning process and accordingly the bulk of safeguarding responsibilities will be discharged trough the delivery of negotiated contracts.
DDCS will, via the Director and delegated responsibility of the DDCS Safeguarding Lead, ensure that Safeguarding is considered during all contract applications & negotiations with consideration to clarity and regard to clear service standards for safeguarding and promoting the welfare of vulnerable adults or children, consistent with local Adults and Children’s Safeguarding Procedures and statutory guidance arising from the Care Act or set out within Working Together to Safeguard Children (2015).
Services and contracting will take account of:
■ Safeguarding responsibilities
■ Cultural diversity
■ The right to family life
■ Due regard to confidentiality in accordance with the sharing information guidance.
■ Appropriate DBS checks for staff
All services are delivered in a non-discriminatory manner, respect the individuality of the adult and are adult centred.
All DDCS Staff are responsible for ensuring that the safeguarding needs of Vulnerable Adults are at the forefront of service delivery; and ensuring that all the services provided meet the quality standards that relate to safeguarding and the six principles set out in section 1. above.
-
Operational Service Delivery Leads - those who oversee the actual delivery of contracted activities arising from DDCS works - should have sufficient knowledge to support all staff with safeguarding adults issues together with the support of the DDCS Safeguarding Lead.
Operational Service Delivery Leads will ensure that all staff take a proactive approach to safeguarding vulnerable adults, are aware of their roles and responsibilities relating to safeguarding vulnerable adults, and that they possess the required level of competencies within the Intercollegiate Document for adults as described above in section 3.
Operational Service Leads will be responsible to ensure that all staff working with Vulnerable adults their families, children and adult or young carers/parents, participate in appropriate safeguarding supervision and safeguarding children training, both of which are mandatory.
At appraisal, Personal Development Plans should reflect that all DDCS staff (both directly employed and subcontracted) continue to meet the safeguarding competencies required for the contractual environment they are employed in and the role they deliver within that context.
Operational Service Leads will be responsible to support HR to ensure that all staff who work with adults, their families and adult carers/parents have an Enhanced Disclosure and Barring Service (DBS) check in line with local commissioning arrangements as required by local commissioners.
They should also be working in accordance with the NSPCC Safer Recruitment practices [1] and Disclosure and Barring Service recruitment standards.
[1] See NSPCC Safer Recruitment
-
All staff must be aware of the following definitions:
Adults Safeguarding
The Statutory Guidance issued under the Care Act, published in October 2014, states that adult safeguarding means ‘protecting an adult’s right to live in safety, free from abuse and neglect’ (Section 14.7).
The purpose of adult safeguarding is to prevent harm and reduce the risk of abuse or neglect to adults with care and support needs.
Care Act factsheets - GOV.UK (www.gov.uk)
Statutory Framework
The statutory framework introduced under the Care Act applies to any person aged 18 or over whom:
■ Has needs for care and support (regardless of the level of need and whether or not the local authority is meeting any of those needs)
■ Is experiencing, or is at risk of abuse or neglect, and
■ As a result of those needs, is unable to protect themselves against the abuse or neglect or the risk of it.
Proportionality
The types and forms of abuse or neglect are broad, and it is important that people err on the side of raising concerns. However growing awareness of adult abuse has led to an increase in reports of concerns and subsequent safeguarding work. Many concerns are directed towards the safeguarding system when they should be dealt with through contractual, managerial, complaints or disciplinary procedures. Some concerns require complex social work case management rather than a formal safeguarding response.
Types of Abuse
Abuse and neglect can take many forms and relate to Ten categories of abuse as documented in the Care Act 2014, these are
■ Physical abuse
■ Domestic violence
■ Sexual abuse
■ Psychological abuse
■ Financial or material abuse
■ Modern slavery
■ Discriminatory abuse
■ Organisational abuse
■ Neglect and acts of omission
■ Self-neglect.
For more details, and indicators see Types of abuse: Safeguarding adults | SCIE
Where staff are aware that an adult has suffered or is at risk of suffering significant harm, a safeguarding adult referral must be considered.
Staff should follow the procedural guidelines associated with this Policy.
Physical Abuse
Physical abuse includes hitting, slapping, pushing, kicking, and misuse of medication, restraint and inappropriate sanctions.
Domestic Violence
Domestic Violence includes psychological, physical, sexual, financial; Honour based violence and Forced marriage.
Sexual Abuse
Sexual abuse includes rape, sexual assault or sexual acts that the vulnerable adult has not consented to or was pressurised into consenting to.
Psychological Abuse
Psychological abuse includes threats of harm or abandonment, deprivation of contact, humiliation, blaming, controlling, intimidation, coercion, harassment, verbal abuse, isolation, discrimination or unequal treatment.
Financial Abuse
Financial or material abuse includes theft, fraud, exploitation, pressure in connection with wills, property, inheritance or financial transactions, the misuse or misappropriation of property, possessions or benefits.
Discriminatory Abuse
Discriminatory abuse includes unequal treatment, verbal abuse, inappropriate and discriminatory use of language, harassment, exclusion, racist, sexist, or homophobic behaviour and incitement of others to discriminate based on difference.
Organisational Abuse
Organisational abuse occurs where the routines and regimes within care settings deny people rights, choices and opportunities. Institutional abuse can be caused by weak or oppressive management, inadequate staffing (numbers, competence), inadequate supervision or support, "closed" communication, lack of knowledge of Whistleblowing policies and lack of training. Indicators of Organisational abuse include:
■ Denial of rights
■ Threats of punishment, loss of personal possessions or eviction in order to gain compliant behaviour
■ Denial of food, drink, adequate clothing and/or suitable living environment
■ Denial of access to friends, family, solicitor, doctor, care manager etc.
■ Denial of access to money; access to information about self, information about rights and responsibilities of the management of the home/service.
Neglect
Neglect and acts of omission includes ignoring medical or physical care needs, failure to provide access to appropriate health, social care or educational services, the withholding of the necessities of life such as medication, adequate nutrition and heating.
Self-Neglect
Self-neglect includes a wide range of behaviour neglecting to care for one’s self with personal hygiene, health and environment including behaviours such as hoarding.
Other Key Adults Safeguarding concepts and Agendas
A non-exhaustive list of other key safeguarding agendas and terms – which can be relevant to both adults and children’s safeguarding are set out below.
Historical Abuse Allegation
Adult clients who disclose they have been abused in the past must be treated sensitively.
Service Users should be offered information, support, counselling and any other available services. However, staff must also consider whether the alleged perpetrator may pose a risk to others.
Where staff feel a child is at risk of harm then they have a duty to refer to children’s social care. DDCS’ ‘Safeguarding Children’ Policy must be followed.
In the event of any concern around a child, staff must contact the DDCS Safeguarding Lead without any avoidable delay who will in turn contact the relevant local safeguarding boards and systems.
Serious Incident (SI) & Serious Case Reviews (SCR)
Some safeguarding concerns may be raised as an Incident and reported via DATIX web. Subsequently they may be subject to a SI. Incidents raised on DATIX that involve abuse or neglect of other Service Users (or potential for such) must also be managed as a safeguarding investigation.
Local Adult Safeguarding Boards must arrange a Safeguarding Adults Review when an adult has died (including suicide) and abuse or neglect are known or suspected to be a factor in the death. The purpose of a SCR is to establish whether there are lessons to be learned from a case about the way in which professionals have worked, what those lessons are and how they will be implemented and monitored.
If an adult subject to a SCR or their alleged abuser, is or has been a Service User of Provide, an Internal Management Review (IMR) will be completed by the Safeguarding Team and supported and monitored by the Head of Safeguarding.
In the event of any SI or SCR the Organisation’s relevant policies must be consulted.
Consent
Learning from high profile inquiries identified recurrent themes in the failures of care and protection:
■ Patients are not empowered to make choices about their care and protection.
■ Patient’s voice is not heard.
■ Neglect and abuse arise in the absence of effective prevention and early warning systems.
It is always essential in safeguarding to consider whether the adult at risk is capable of giving informed consent in all aspects of their life. If they are able, their consent should be sought. This may be in relation to whether they give consent to:
An activity that may be abusive and consent to abuse or neglect was given under duress (e.g. as a result of exploitation, pressure, fear or intimidation), then staff member must consult with the line manager or Safeguarding Team as in this event consent can be disregarded.
A safeguarding adult’s investigation/assessment in response to a concern that has been raised. Where an adult at risk with capacity has made a decision that they do not want action to be taken and there are no public interest or vital interest considerations, their wishes must be respected. The person must be given information and have the opportunity to consider all risks and fully understand the likely consequences of that decision over the short and long term.
■ The recommendations of an individual protection plan being put in place.
■ A medical examination.
■ An interview.
■ Certain decisions and actions taken during the safeguarding adult process with the person or with people who know about their abuse and its impact on the adult at risk - If, after discussion with the adult at risk who has mental capacity, they refuse any intervention, their wishes will be respected unless under the MCA
■ There is an aspect of public interest (e.g. not acting will put other adults or children at risk).
■ There is a duty of care on a particular agency to intervene for example the Police (if a crime has been or may be committed).
If the Service User lacks capacity to consent to a safeguarding investigation (see Safeguarding Adults Executive Board’s Guidance) and is un-befriended, or their friend or family is their alleged abuser or alleged victim, then an Independent Mental Capacity Advocate (IMCA) must be provided.
The IMCA can be accessed by sending the completed MCA2 form to the Safeguarding Team, and informing them of the need for an IMCA referral. Following discussion with the safeguarding team a referral should be made to the IMCA service as advised. See Independent Mental Capacity Advocate (IMCA) | SCIE
Honour Based Abuse
“Honour” based abuse is a complex issue which is deeply embedded in the culture of some families and communities. It is important to understand that honour must never be accepted as a rationale for inappropriate and abuse behaviour. This form of violence refers to specific forms of abuse based on control of social, sexual and lifestyle choices, the concept of honour being closely linked to control of females (mainly) or males. It is now a statutory requirement that Health Organisations address issues of HBA, Forced Marriage and Female Genital Mutilation (The Right to Choose; HM 2008)
All staff should be aware of cultural issues when HBA is disclosed or identified. If a client discloses HBA then appropriate responses should be provided by the Health Professional. It is important that client’s safety is always considered. Health Staff must always seek the advice of the DDCS Safeguarding Lead.
If there is a language barrier, family members of friends of the victim must never be used as interpreters. If the Service User is under the age of 18 then the DDCS ‘Safeguarding Children Policy’ must be followed.
Forced Marriage
Forced Marriage is an abuse of human rights. “Marriage shall be entered into only with the free and full consent of the intending spouses” (Universal Declaration of Human Rights, Article 16, 2; UN 1948). Forced Marriage is a form of domestic abuse and depending on age of the victim a form of child abuse. Some Forced Marriages involve a partner coming from overseas or a British Citizen being sent abroad to be married. It is now recognised that health staff are sometime ideally placed to provide early and effective interventions.
Female Genital Mutilation
Female Genital Mutilation is the collective term used for procedures which include the partial or total removal of the external female genital organs for cultural or other non-therapeutic reasons.
The Prohibition of Female Circumcision Act 1985 made this practice illegal in this country.
The Female Genital Mutilation Act 2003 replaced the 1985 Act and it is now illegal for girls to be taken abroad for this procedure. In 2011 the Home Office published Multi Agency Practice Guidelines, which is available on: www.homeoffice.gov.uk/publications/crime/FGM
Duties & Responsibilities for HBA, FGM and Domestic Abuse
DDCS has a responsibility for safeguarding children and protecting vulnerable adults or victims of HBA, FGM, Forced marriage and Domestic Abuse (HM Government 2009).
The policy is relevant to both adult and child victims.
HBA and Forced Marriage can claim both male and female victims and the principles of care can be adapted across gender or sexual orientation. It is important to understand that forced Marriage and FGM are all forms of domestic abuse/child abuse depending on the age of the victim.
Therefore, all have a statutory duty to respond to these forms of abuse and follow policy and guidelines to comply with safeguarding requirements.
Principles of care can also be adapted to meet the needs of victims who may have added vulnerabilities such as learning difficulty, mental illness and sensory impairment. Health Staff should always seek specialist advice from the Safeguarding Team when dealing with abuse that involves HBA, FGM or Forced Marriage.
Processes, Record Keeping and Confidentiality in HBA
Processes which support effective and safe responses, and which do not increase risk of dangers faced by victims include:
■ Effective Inter Agency Working
■ Risk Assessment
■ Appropriate Record Keeping
Basic Details should be recorded appropriately and should include, name dates of birth and a short description of the incident, or allegation. They should then state that it involves “Honour Based Abuse” and enquiries referred on to the Safeguarding Team.
All staff must ensure clear concise records of discussions, decisions and actions must be recorded contemporaneously with a date, name and signature.
All recordings should be based on fact or professional opinion and kept in the client’s records.
All assessments must consistently assess and record the racial linguistic and religious identity and needs of the Service User and their family.
The records of clients are known to be subject to an Adult Protection Plan should indicate this clearly.
Records of on-going investigation and management of on-going incidents must be recorded in a secure manner agreed with the victim and all the professionals involved.
Consideration should be given to restricting access to the information.
Always consider who this information shared with at any level and only provide information on a need-to-know basis.
All staff within DDCS have a responsibility to:
■ Be alert to the potential warning signs of Honour Based Abuse, Forced Marriage and Female Genital Mutilation and to consider this as a possibility.
■ Take a proactive role in establishing if these forms of abuse are an issue and to be aware of the appropriate actions to take if a disclosure is made.
■ Be aware of confidentiality issues and when to make a disclosure without the victim’s consent, including identified child protection or vulnerable adult concerns.
■ Attend training and keep updated with regard to both forced marriage and the wider domestic abuse agenda.
In many cases an interview with a health professional may be the victim’s only chance to tell someone what is happening. All working with victims of Forced Marriage and HBA need to be aware of the ‘One chance rule’ and only have one chance to speak to a potential victim thus only one chance to save a life. This means that all working with statutory agencies need to be aware of their responsibilities and obligations when they identify HBA. If the victim is allowed to walk out of the door and away from the practitioner, without support being offer, that “one chance” might be lost.
Organisational Abuse
Organisational abuse occurs where the culture of an organisation (a hospital, health care provider, a ward, a care home, a nursing home etc.) places emphasis on the running of the establishment and the needs of the staff above the needs and care of the vulnerable person.
Abuse by an organisation when imposing firm and insensitive routines; poor practices embedded in systems, unskilled, intrusive or invasive interventions; or an environment allowing inadequate privacy or physical comfort.
In the event of any DDCS staff identifying any of these in the course of their duties, they must ensure Service Users safety and escalate this to line management this to their Line Manager, DDCS Safeguarding Lead and DDCS Director without any avoidable delay. If these actions are taken and the risks remain unchanged or the matter is so serious that the staff cannot discuss this with any of the above, then the DDCS Whistleblowing Policy must be followed.
Where a health professional identifies a vulnerable adult living in accommodation where they may potentially be at greater risk of significant harm or exploitation because the provider is unregulated and providing a service to a number of adults who are or could be either eligible or in receipt of community care services– such as within a bed and breakfast establishment–they have a duty to notify both the DDCS Safeguarding Lead and the Local Authority’s Adult Safeguarding Unit.
The health professional who receives or raises an alert in relation to an institutional abuse investigation must immediately contact (within 24 hours maximum):
■ DDCS Safeguarding Lead.
■ Their Line Manager & DDCS Director.
The health professional must identify the names of any other vulnerable adults who may be at risk and ensure that this information is promptly made available to the DDCS Safeguarding Lead so this can be escalated to the Local Commissioners and Local Authority.
Confidentiality & Information Sharing
Where there is potential risk to life and limb, the welfare of the adult is paramount. In such circumstances, the duty to maintain confidentiality is over-ridden by a duty in the public interest (Public Interest Act 1998). Staff have a duty to pass on information relating to suspected adult abuse to Police.
Consent is not required to make a safeguarding referral where:
There is significant risk of harm for the Service User or other vulnerable adults and seeking permission is likely to increase risk to the adult.
Permission has been refused previously but sufficient professional concern remains to justify disclosure.
Seeking permission is likely to impede a criminal investigation.
There is significant risk to others (including children and young people under the age of 18).
Children who may be the subject of abuse.
Failure to disclose information may expose the Service User or others to risk of death or serious harm.
Information should be shared on a need-to-know basis. Staff should consult their line manager or Safeguarding Lead for advice if they are unsure.
Police must be informed about allegations of a crime at the earliest opportunity. Staff should discuss this with the Police Domestic Violence and hate Crime Units (DVHC). The local Police’s contact details can be obtained by dialling 101 or from the Local Authority.
Visiting Vulnerable Service Users
Visits to vulnerable Service Users who may lack capacity to consent to a visit from an alleged perpetrator should only take place following an MCA Assessment and a decision that such a visit would be in the best interests. Decisions to allow such visits should be regularly reviewed.
-
All Staff have a key role to play in actively promoting the health and wellbeing of people. Section 11 of the Children Act 2004 places a duty on all providers of NHS services in so much that they have regard to the need to safeguard and promote the welfare of children.
All health professionals who work with adults, children, and families should be able to:
■ Understand the risk factors and recognise children in need of support and/or safeguarding
■ Recognise the needs of parents who may need extra help in bringing up their children and know where to refer for help
■ Recognise the risks of abuse to an unborn child
■ Contribute to enquiries from other professionals about adults and their family or carers
■ Liaise closely with other agencies, including other health professionals
■ Assess the needs of adults and the capacity of parents/carers to meet their needs
■ Plan and respond to the needs of adults and their families, particularly those who are vulnerable
■ Contribute to child protection conferences, family group conferences and strategy discussions
■ Contribute to planning support for adults at risk of significant harm, e.g., adults living in households with domestic violence or substance misuse
■ Help ensure that adults who have been abused and parents under stress (e.g., those who have mental health problems) have access to services to support them
■ Play an active part, in safeguarding adults from significant harm
■ As part of generally safeguarding adults, children, and young people, providing ongoing promotional and preventative support, through proactive work with children, families, and expectant parents
■ Contribute to serious case reviews (SCRs) and their implementation
-
Evidence suggests that adults, children, and their families who receive coordinated early help are less likely to develop difficulties that require intervention through a statutory assessment under the Children Act 1989.
Adults, children, young people and families experience a range of needs at different times in their lives. See Safeguarding Adults Executive Board’s Guidance on Referring a Safeguarding Adults Concern for further information.
Confidentiality and Data protection must be taken seriously while sharing information and making referrals. However, this should not be a barrier to safeguard an adult, child, or a young person.
-
Where there are significant concerns about the safety of a vulnerable adult, professionals should contact 999 or Local Council Adult Social Care teams.
Any discussion, referral and advice must be recorded appropriately in clinical records.
When making a referral staff must:
■ inform the social services whether just requesting advice or making a referral.
■ confirm that they are speaking to an appropriate person who can take the referral, record their name and position.
■ have the appropriate facts to hand to make a clear referral statement.
The guidance that follows does not replace that contained within the Local Safeguarding Adults Guidance; rather it provides a succinct summary of the process. Where there is immediate risk, you must keep the adult safe and where a crime may have been committed, you must call the Police (either using 999 in an emergency, or their local number to contact the Domestic Violence and Hate Crime Unit). Beware not to interfere with any potential evidence – this includes facilitating a Service User to wash or to have their clothes washed. Ensure the Director and Safeguarding Lead are promptly informed.
If you have concerns that an adult is or may be at risk of significant harm from others, then you must complete the appropriate form. Completed forms must be sent to the appropriate Local Authority without any delay and a copy of this must be sent to the Local Adult Safeguarding Team.
There are four key stages for the adult safeguarding process outlined by the Safeguarding Adults Executive Board’s (SAEB’s) Multi-Agency Adult Safeguarding Procedure:
1. Concerns
The initial expressed concern for a vulnerable adult can be raised by professionals, family, friends or other concerned individuals, either in-person, by telephone, email or letter.
They may also be raised through specific organisation processes for example London Ambulance Notifications and police Merlin Adult Come to Notice (ACN) reports. Merlin ACNs are reports completed by operational police officers and sent to local authorities where they have concerns about potential at-risk adults, whether they are a victim, witness, suspect or member of the public. The police will make a decision about whether to refer to the Local Authority, using their operational toolkit. Some concerns may not sit under adult safeguarding processes but remain concerns that may require other action. All concerns should be responded to, and SABs should be satisfied that concerns are being addressed appropriately through their oversight of safeguarding practice.
If, based on the information available, it appears that the following three steps are met, a referral must be made to the Local Authority;
■ A person has care and support needs
■ They may be experiencing or at risk of abuse and neglect
■ They are unable to protect themselves from that abuse and neglect because of those care and support needs.
2. Enquiry
Initial conversation: same day concern received if not already taken place.
Planning meeting: within 5 working days.
Enquiry actions: Target time within 20 working days.
Agreeing outcomes: Within 5 working days of enquiry report.
The Local Authority must make or arrange an enquiry under Section 42 of the Care Act 2014. ‘The Local Authority must make (or cause to be made) whatever enquiries it thinks necessary to enable it to decide whether any action should be taken in the adult’s case (whether under this Part or otherwise) and, if so, what and by whom.’
Where the circumstances are not such as to trigger the Section 42 safeguarding duty, the Local Authority may choose to carry out proportionate safeguarding enquiries, to promote the adult’s well-being and to support preventative action. An enquiry should establish whether and what action needs to be taken to prevent or stop abuse or neglect. Local Authorities should aim to provide swift and personalised safeguarding responses, involving the adult at risk in the decision-making process as far as possible. A report should be collated and drawn up by the Enquiry Officer overseen by the Enquiry Lead.
All enquiries should have established outcomes that determine the effectiveness of interventions. These decisions are made by the SAM in consultation with the adult and other parties involved in the enquiry.
3. Safeguarding Plan and Review
Safeguarding Plan: Within 5 working days of enquiry report.
Review: Not more than 3 months, but dependent upon risk.
Enquiry report outcomes and recommendations are formalised into a Safeguarding Plan.
The plan should outline the roles and responsibilities of all individuals and agencies involved and should identify the lead professional who will monitor and review the plan, and when this will happen. Adult safeguarding plans should be person-centred and outcome focused. Safeguarding plans should be made with the full participation of the adult at risk.
Reviews of adult safeguarding plans, and decisions about plans should be communicated and agreed with the adult at risk. Following the review process, it may be determined that:
■ The adult safeguarding plan is no longer required; or
■ The adult safeguarding plan needs to continue.
4. Closing the Enquiry
Actions immediately following decision to close where possible. Other actions within 5 working days.
The adult safeguarding process may be closed but other processes may continue, for example, a disciplinary or professional body investigation. These processes may take some time.
Consideration may need to be given to the impact of these on the adult and how this will be monitored. Where there are outstanding criminal investigations and pending court actions, the adult safeguarding process can also be closed providing that the adult is safeguarded.
All closures no matter at what stage are subject to an evaluation of outcomes by the adult at risk. If the adult at risk disagrees with the decision to close safeguarding down their reasons should be fully explored and alternatives offered.
Staff who are aware that a vulnerable adult is subject to a safeguarding adults investigation or adult protection plan fails to attend an appointment with DDCS services, should inform the referrer, line manager and consider a further safeguarding referral or the sharing of information with the local Police.
When a member of staff is not entirely satisfied with the clinical, social or emotional picture that is presented or where maltreatment is suspected they must contact the DDCS Safeguarding Lead for advice.
Where Alleged Abusers & Alleged Victims are Both Service Users
It is important that consideration be given to a co-ordinated approach and partnership working, where it is identified that both the alleged abuser and alleged victim are Service Users. Where both parties are receiving a service from the DDCS staff including doctors should discuss cases and consider a joint assessment and support plan where appropriate.
-
Concern or disagreement may arise over another professional’s decisions, actions or lack of actions, in relation to a referral, an assessment or an enquiry. Overwhelmingly these will involve the lead agencies and universal healthcare providers from acute or community settings, and the role of DDCS is likely to be that of providing supportive input rather than initiating and or convening its own multiagency processes or initiating and coordinating actions enquiries where legislative and guidance points to other elements of the multi-agency environment for the key responsibilities.
It is important to note and adhere to the following principles that inform the wider system responses and the issues that may occur in the multi-agency environment: where DDCS may have a role:
■ The safety of individual vulnerable person/adult is the paramount consideration in any professional disagreement, and any unresolved issues should be escalated.
■ Avoid professional disputes that put adults at risk or obscure the focus of the adult
■ Resolve difficulties (within and) between agencies quickly and openly
■ Identify problem areas in working together where there is a lack of clarity and to promote resolution via amendment to protocols and procedures.
Disagreement may also arise regarding response to a referral made to Social Care, e.g.:
■ whether eligibility criteria are met
■ whether concerns justify a particular course of action/enquiry
■ whether to convene an initial case conference - invitation to participate in one should never be a source of disagreement – if an invitation is offered it must be accepted by DDCS.
Dissent can also arise regarding decisions made at case conferences or subsequently regarding implementation of an adult safeguarding plan. If a local resolution cannot be agreed, then this must be escalated to more senior staff with wider experience of safeguarding concerns. In the context of DDCS, this is unlikely to arise as the flat structure of the organisation and direct involvement in safeguarding discussions of the DDCS Safeguarding Lead will provide appropriate seniority and experience for DDCS to engage with any escalation of concerns that may occur.
-
DDCS will make every effort to ensure safe recruitment of all staff. However, in an unfortunate event where there is an accusation of abuse against an DDCS Employee or subcontractor the Director and the Safeguarding Lead must be notified. The DDCS employment processes – including ‘Disciplinary Procedure’ and any contractual requirements flowing from commissioned works must be followed.
Crucially, appropriate referrals to Local Adults Social Care will be enacted within the timeframes stipulated and Local Authority & Adults Safeguarding systems will be informed.
This can apply when a member of staff has:
■ Behaved in a way that has or may have harmed a Vulnerable Adult
■ Possibly committed a criminal offence against or related to a Vulnerable Adult
■ Behaved towards a Vulnerable Adult in a way which indicates he/she is unsuitable to work with Vulnerable Adults.
If the Employee or subcontractor has allegedly committed a criminal offence:
■ The Director and Safeguarding Lead must be contacted without delay and if necessary the local Police must be contacted.
■ If the allegation is against the Director and Safeguarding Lead, then the local safeguarding system leads must be notified.
■ Where any concerns regarding an employee’s suitability to work with children or vulnerable adults is identified, the employer must refer the case to the DBS and any relevant professional body.
DDCS will work together with local authority social care and/or other partners to protect the Vulnerable Adult. DDCS must consider the impact on the Vulnerable Adult concerned and provide support as appropriate. Liaison between the agencies should take place to ensure that the adult’s needs are addressed.
If DDCS staff or subcontractors becomes aware of any information regarding another member of DDCS staff or contractors which identifies that an adult may be at risk of harm or has been harmed (including the member of staff’s own partner, relatives, or friends), they must immediately report this information to their line manager and make referral to the social services/police if necessary.
The information must also be shared with the DDCS Safeguarding Lead for who will be responsible for sharing appropriately within DDCS as well as notifying Social Care and LADO and or Police as appropriate. As with all investigations, a police / criminal line of enquiry will take precedence above all others.
Safeguarding Concern about a Service User of DDCS
In the event of any safeguarding referral made to a Local Authority about a Service User, must be escalated to the Director and DDCS Safeguarding Lead without any delay.
The department must ensure every aspect of raised concerns and referral is taken seriously and investigated thoroughly. Immediate action must be taken to ensure Service Users safety.
The Service User/family/carer will be informed about the raised concerns appropriately to improve safety and the quality of service. The responsibility lies with the Service Delivery Operational Lead and DDCS Safeguarding Lead to contact the Service User.
Where possible and appropriate, Service User/family/carer will be involved in the investigation and action plan. A key aim should be ‘to let the Service User drive the organisation’. This will ensure Provides values and missions to listen and work together for a better outcome for our Service Users are achieved. Under the Care Act 2014, the individual who concern was raised for must be involved in the investigation and the investigator should always contact them and discuss the raised alert and how they wish things to proceed.
The DDCS Safeguarding Lead will work closely with the Local Authority and the appropriate department where concerns were raised to complete an investigation with the Director’s support throughout the investigation procedures.
Completed investigations with action plans will be sent to DDCS Executive Leadership.
-
All staff that work with children should ensure that they have the skills and knowledge as set out in ‘Intercollegiate Document’ as described in section 2 above.
Vulnerable Adults Safeguarding Awareness must be covered within the DDCS induction for all new staff, and sub-contractors and new staff should also receive additional local introductory training in safeguarding children from their supervisor/ line manager. At Induction Training all DDCS staff must be informed of the Vulnerable Adults Safeguarding Policy and Guidelines.
All DDCS staff must receive training and regular updates at the appropriate level for their role. It is mandatory for all staff working with adults, children, families, and parents/carers of children to attend training updates.
All staff must ensure that they are aware of their responsibility to attend safeguarding adults training in accordance with local training Policy and familiarise themselves with the DDCS training arrangements.
Any member of staff unsure of their training needs should contact the DDCS Safeguarding Lead to discuss their requirements.
A note on supervision
Vulnerable Adults Safeguarding supervision is mandatory for all health professionals working with children and their families. Currently DDCS staff do not deliver work of the nature and the following is a suggested text should DDCS ever require that supervision structures are established to support safeguarding works not currently delivered.
In general, a proactive approach to supervision is required to ensure that all staff are supported and continue to develop their skills and knowledge in recognising and acting on concerns regarding the safeguarding of Vulnerable Adults (or children) and responding to their needs.
■ Operational Service Delivery Leads must ensure that protected time is available to enable staff to receive supervision in accordance with the guidelines.
■ Vulnerable Adults safeguarding support, and supervision will be provided in addition to clinical supervision and management supervision.
■ The DDCS Safeguarding Lead can provide supervision – but not clinical supervision - to encourage reflection, development and support for DDCS staff.
Supervision arrangements will be reviewed in line with the consideration of contracted and commissioned services as set out above in section 1. and 6. above.
-
Care Act (2014): Act of Parliament, UK Stationery Office.
Care Quality Commission (2010) Standards for Safeguarding, Risk
Management Standards: http://www.cqc.org.uk
Care Quality Commission; Our Safeguarding Protocol; The Care Quality Commission’s Commitment to safeguarding.
Children Act (2004): www.legislation.gov.uk
Civil Protection Act (2007): Forced Marriage: HM Government
Department of Health: No Secrets (2000) Guidance on Developing and Implementing Multi Agency Policies and Procedures to Protect Vulnerable Adults from Abuse-DH.
DBS (2014): https://www.gov.uk/disclosure-barring-service-check/overview
Safeguarding Adult Executive Board: https://www.saeb.org.uk/
FGM Act (2003): www.legislation.gov.uk/ukpga/2003/31/contents
Multi Agency Practice Guidelines (2009) Handling cases of forced marriage: HM Government.
Protecting Vulnerable Adults: Waltham Forest Council (2013): www.walthamforest.gov.uk
Redbridge Safeguarding Adults (2011): Working documents. London Borough of Redbridge.
The Right to Choose (2008): Multi Agency statutory guidance: HM Government.
The Public Interest Disclosure Act (1998): www.legislation.gov.uk
UN (1948) The Universal Declaration of Human Rights: www.un.org/en/documents/
Table 1: Core Principles of the Care Act 2014
Children
Section 11 of the Children’s Act 2004 and the wide range of statutory responsibilities set out in Working Together to Safeguard Children (2023) set out a range of responsibilities and functions for the safeguarding, and ongoing promotion of welfare and protection of children and young people.
The safeguarding and promotion of the welfare of children is an integral element of the services and care offered to all children and their families by all staff in both statutory and voluntary and community sector organisations working on behalf of Dan Devitt Consultancy Services (DDCS).
The service offer delivered via or on behalf of DDCS is potentially very broad in nature and could include care offered to children, young people, families or adults who are parents or carers.
The aim of the policy is to ensure that there is a robust system in place to safeguard children and young people who receive service from DDCS and to support staff with safeguarding children and young people. The policy sets out the roles and responsibilities of all staff and those working on behalf of DDCS with respect to keeping children safe and promoting their welfare.
-
Dan Devitt Consultancy Services does not currently or foreseeably have any direct contracted or subcontracted relationship or operate on its own as either a provider of services to the community where direct care or clinical provision to children and young people (CYP) would be conducted.
That limitation on the scope of activities delivered by DDCS notwithstanding this policy has been drafted to ensure that DDCS is well-placed to ensure that it is delivering a comprehensive approach to Safeguarding CYP and related policies, and able to adapt to future changes in commissioned activities. It stands as a visible sign of DDCS’ awareness of and commitment to the provision of safeguarding and related assurance for services that are delivered through DDCS via subcontracted entities and with a view to ensuring compliance is built into the DDCS policy framework before rather than after it becomes necessary.
DDCS’ work varies in scope across counties and local NHS Trusts, creating relationships between DDCS and Local authorities, NHS, public health providers, and other relevant organisations.
These organisations do not currently perform functions where children’s safeguarding (or adults) functions are entailed, but this is a situation that could potentially change over time.
To provide assurance of DDCS’ robust and forward-thinking approach to safeguarding this policy and others on different safeguarding themes have been drafted in preparation in case any of the functions do, one day, become an element of DDCS business.
DDCS will ensure that it monitors and provides assurance to its commissioners that its relationships – either to commissioning bodies or subcontracted entities - align with its commitment and obligations and accountability to commissioners for safeguarding practice and policies in subcontractors.
This will be reviewed on a regular and ongoing basis and especially at the commencement of new contractual relationships where an assessment to ensure a full compliance with relevant safeguarding practice and policies is conducted.
In this way, DDCS will evolve its safeguarding response in line with future requirements whilst constantly assessing, reflecting upon and improving its safeguarding approach and policy suite.
-
The Children Act 1989 provides a comprehensive framework for the care and protection of children and young people.
The fundamental principle that underpins the Children Act is that the welfare of the child/young person (under 18 years) is paramount.
Achieving positive outcomes for children requires all those with responsibility for assessment and provision of services to work together according to an agreed plan of action.
In addition, the Children Act 2004 (Section 11) sets out duties for a wide range of bodies including health. Therefore, health agencies, including those contracted or subcontracted to deliver health functions (as with Local Authority Public Health contracted community services – including those commissioned via community pharmacies) which have a statutory duty to carry out their functions with an explicit focus on the need to the need to safeguard and promote the welfare of children and young people. This duty extends to both directly contracted and delivered and subcontracted services.
“Working Together to Safeguard Children” (DH 2015) statutory guidance sets out how organisations and individuals should work together to safeguard and promote the welfare of children.
The Safeguarding Children & Young People Policy and Guidelines complement and should be used in conjunction with Local Safeguarding Procedures for the geographical region(s) where DDCS operations and contracted activities are being delivered. Currently services are being delivered in London and should adhere to the London Safeguarding Children Core Procedures but this and the links to other areas procedures will be assessed on an ongoing basis. Core resources are available, via the link below:
London Safeguarding Children Partnership’s Core Procedures and Practice Guidance.
The Policy is intended to support all DDCS staff and subcontractors working on behalf of DDCS with safeguarding children within all geographical areas in which services are delivered.
The Intercollegiate Document ‘Safeguarding Children Roles and Competencies for Healthcare Staff Intercollegiate Document’, (RCN 2019), sets out the levels of competencies expected of all staff working within the health service.
All staff must ensure that they possess the required knowledge, skills and competencies – in line with their role as set out in their training matrix in line with the Intercollegiate Document (2019).
-
The purpose of this policy is to ensure that DDCS Staff and subcontracted entities are able to appropriately fulfil their safeguarding obligations with regards to children and young people.
DDCS understands that the safety, rights and wellbeing of service users is paramount and that they have a right to feel safe and protected from any situation or practice that results in them being harmed or at risk of harm. DDCS is committed to ensuring the primacy of service users human rights, choice; and their right to control and be included in care/decision making.
DDCS understands these are important for meeting the individual needs of service users and reducing the potential for abuse. It is therefore central to the DDCS Safeguarding response.
A note on Equality and Diversity
This policy has been developed in line with DDCS’ principles of Equality and Diversity and is underpinned by the following standards:
■ An adult’s welfare and safety is everyone’s responsibility.
■ Staff must work together, understand and appreciate other professionals’ roles and responsibilities.
■ No one must be discriminated against on the grounds of age, race, ethnicity, religion, culture, class, sexual orientation, gender, gender reassignment or disability.
-
The policy applies to all staff employed or working on behalf of DDCS. This includes those that are:
■ Full or Part Time directly employed staff
■ Executive Leadership supporting DDCS
■ Temporary, voluntary, contracted or self-employed staff
■ Consultants and agency staff
The above will be referred to as ‘all staff’ in the policy.
-
All Staff
All staff must always be alert to the possibility of significant harm to children through abuse or neglect, or to a child who is ‘in need’. All staff should be able to recognise indicators and know how to act upon concerns, their depth of knowledge being commensurate with their roles and responsibilities.
Effective safeguarding arrangements should aim to meet the following two key principles:
■ Safeguarding is everyone's responsibility: for services to be effective each individual and organisation should play their full part; and
■ A child centred approach: for services to be effective they should be based on a clear understanding of the needs and views of children.
All staff must be aware of
■ the vulnerabilities of certain groups of children such as those who are disabled, ‘looked after’, privately fostered and socially excluded.
■ the vulnerabilities of certain groups of adults who may find parenting difficult.
The latter category can include a very wide range of people and touch upon a broad range of conditions, and agendas. For example, those experiencing domestic abuse, coercive control and/or violence, instability arising from complexity involving mental health conditions or problems, uncontrolled substance or alcohol misuse, learning disabilities, involvement with the justice system or exposure to the effects of criminality, violence and the drugs trade, or those with unmet support needs and those exposed to economic adversity, poverty and stresses arising from the cost-of-living crisis.
Core Principles
All staff must therefore be aware of relevant adult safeguarding policies and procedures which may be involved including where incidents of children and young people potentially abusing vulnerable parents or carers.
All staff working primarily with adults who are parents or carers should always consider the effects on parenting capacity and subsequent implications for children of the adult’s illness or behaviour.
All staff must recognise that sharing information is vital for early intervention to ensure that children are protected from abuse and neglect and that the safeguarding of children is paramount and can override any duty of confidentiality.
All staff regardless of grade or position must follow local SCB Procedures where there are concerns that a child is being abused or when there are child protection concerns. This cannot be delegated to others.
All staff should be aware that when they have concerns about possible child abuse or neglect, they can discuss their concerns with the DDCS Safeguarding Lead or a Local Safeguarding Children Board advisor or local NHS Named/Designated Safeguarding Professional, Manager or Supervisor, as required and must know how to access this support.
IN EMERGENCIES
If emergency action is needed to protect an adult this should never be delayed due to the need to discuss concerns.
See below for the process for actioning immediate concerns as referenced in the HM Gov Guidance: Report Child Abuse.
Key contacts and numbers to discuss a child’s safeguarding issue:
■ If a child or young person is in immediate danger, call 999.
■ If you're worried that a child is being abused or neglected, contact the children’s social care team at their local council. You can find a collected list of London’s Local Safeguarding Contacts here.
■ You can also call the NSPCC on 0808 800 5000 to discuss concerns. This phone line is open 10am–4pm Monday to Friday.
All staff should uphold the rights of the child to be able to communicate, be heard and safeguarded from harm and exploitation whatever their race, religion, language, ethnicity, gender, sexuality, age, health or disability, location/placement, criminal behaviour, political or immigration status.
Those who work directly with children/young people should also have access to the Local SCB Child Protection procedures (See London Safeguarding Children Partnership – Safeguarding Core Procedures and Practice Guidance). LSCB Procedures available electronically so If staff print or save copies, they are responsible for ensuring these remain updated.
All staff must undertake mandatory child protection/safeguarding training at a level that is appropriate for their role and commensurate with the operational requirements of their post for which they are employed and reflects the competencies within the Intercollegiate Guidelines as set out in Safeguarding Children and Young People: Roles and Competencies for Healthcare Staff (RCN 2019).
All staff must ensure that they update their skills and knowledge by undertaking further refresher training as appropriate and in line with level of competency.
Assurance of this compliance will be through an annual audit process delivered by the DDCS Safeguarding Lead and assured by the DDCS Director. This will be refreshed in line with contractual obligations rather than strictly by calendar year to ensure that assurance is quickly developed for new areas of operation or focus, rather than waiting on a calendar bound process.
All staff that work with children should also ensure that they have the skills and knowledge as set out in ‘Common Core of Skills and Knowledge for the Children’s Workforce’ (DfES 2005). See the Association of Directors of Children’s’ Services factsheet for an overview.
All staff that work regularly with children are responsible for ensuring that they access on going safeguarding children supervision depending on the recommendations for the practice area.
DDCS Director
The DDCS Director has overall responsibility for ensuring that the DDCS contribution for safeguarding and promoting the welfare of children is discharged effectively for all children & young people for whom DDCS delivers services. This includes ensuring that:
■ There are safe and robust operational arrangements in place for safeguarding children in all the services that are provided.
■ Staff work in line with Local Child Protection Procedures, and any other locally agreed policies and guidance.
Operational responsibility for maintenance and updates to the policy are delegated by the Director to the DDCS Safeguarding Lead and the Safeguarding Lead’s performance is assured by the Director.
DDCS Safeguarding Lead
The DDCS Safeguarding Lead provides professional leadership and strategic direction on DDCS safeguarding children-related activities or services to provide a coordinated and integrated safeguarding service that evolves in time with DDCS.
It is the responsibility of the DDCS Safeguarding Lead to ensure that contracted services are delivered in accordance with the Safeguarding Children Policy and Guidelines and that there are safe systems and processes in place to support DDCS contracted services.
The DDCS Safeguarding Lead is responsible for ensuring that the needs of all children and young people are at the forefront of DDCS delivery planning and contractual negotiations and that high quality health services that meet identified quality standards are delivered.
The DDCS Safeguarding Lead will ensure that monitoring and reporting of safeguarding activity to fulfil the relevant and appropriate requirements under Working Together to Safeguard Children (2015), CQC Essential Standard of quality and safety (2010), Standard 5 of the Children’s National Framework and recommendations from Serious Case Reviews takes place.
The DDCS Safeguarding Lead is responsible for promoting good professional practice and providing specialist advice and support to DDCS staff and subcontractors on any issue relating to safeguarding children.
The DDCS Safeguarding Lead will ensure provision of safeguarding children supervision and training to staff, regular audits of practice and conduct the internal Management Reviews (IMR’s) as part of Serious Case Reviews or under a regular audit or to investigate an incident.
The DDCS Safeguarding Lead will ensure that DDCS is represented at the health subgroup of the local Safeguarding Children Board when necessary (LSCB).
DDCS Contracting functions
DDCS exists (as set out in the Introduction above) to provide commissioned services and contracting arrangements that cannot be easily fulfilled by the constitutional structure of organisational environment in a particular circumstance. As a result of this DDCS is involved explicitly in the contracting and commissioning process, and accordingly the bulk of safeguarding responsibilities will be discharged through the delivery of negotiated contracts.
DDCS will, via the Director and delegated responsibility of the DDCS Safeguarding Lead, ensure that Safeguarding is considered during all contract applications & negotiations with consideration to clarity and regard to clear service standards for safeguarding and promoting the welfare of children, consistent with local Children Safeguarding Procedures and statutory guidance within Working Together to Safeguard Children (2015).
Services and contracting will take account of:
■ Safeguarding responsibilities
■ Cultural diversity
■ The right to family life
■ Due regard to confidentiality in accordance with the sharing information guidance
■ Appropriate DBS checks for staff
All services are delivered in a non-discriminatory manner, respect the individuality of the child and are child centred.
All DDCS Staff are responsible for ensuring that the safeguarding needs of children are at the forefront of service delivery; also ensuring that all the services provided meet the quality standards that relate to safeguarding and the five outcomes for children (Every Child Matters: Change for Children Programme, 2006).
Operational Service Delivery Leads
Operational Service Delivery Leads - those who oversee the actual delivery of contracted activities arising from DDCS works - should have sufficient knowledge to support all staff with safeguarding children issues together with the support of the DDCS Safeguarding Lead.
Operational Service Delivery Leads will ensure that all staff take a proactive approach to safeguarding children, are aware of their roles and responsibilities relating to safeguarding children, and that they possess the required level of competencies within the Intercollegiate Document as described above in section 2.
Operational Service Leads will be responsible to ensure that all staff working with children, their families and adult carers/parents, participate in safeguarding children supervision and safeguarding children training both of which are mandatory.
At appraisal, Personal Development Plans should reflect that all DDCS staff (both directly employed and subcontracted) continue to meet the safeguarding competencies required for the contractual environment they are employed in and the role they deliver within that context.
Operational Service Leads will be responsible to support HR to ensure that all staff who work with children, their families and adult carers/parents have an Enhanced Disclosure and Barring Service (DBS) check in line with local commissioning arrangements as required by local commissioners and in line with local Safeguarding Children Board (SCB) procedures and that this is reviewed every 3 years.
They should also be working in accordance with the NSPCC Safer Recruitment practices [1] and Disclosure and Barring Service recruitment standards.
[1] See NSPCC Safer Recruitment
-
All staff must be aware of the following definitions:
Child Abuse
Child abuse is defined by Working Together (2015) as ‘a form of maltreatment of a child (under the age of 18 – i.e.,17 years and 364 days old). Somebody may abuse or neglect a child by inflicting harm, or by failing to act to prevent harm. Children may be abused in a family or in an institutional or community setting by those known to them or, more rarely, by others (e.g., via the internet). They may be abused by an adult or adults, or another child or children’.
See Working together to safeguard children - GOV.UK (www.gov.uk)
Physical Abuse
Physical abuse is when someone physically hurts a child or young person on purpose. Physical abuse can include: hitting; shaking; poisoning; burning; drowning; suffocating. This may also be caused when a parent fabricates the symptoms of, or deliberately induces illness in a child.
Emotional Abuse
Examples of emotional abuse include being made to feel worthless, wrong or unhappy; being unfairly blamed; being bullied; being made to feel frightened or in danger; seeing or hearing domestic violence within the home. Emotional Abuse can damage self-esteem and severely affect friendships, school and home life.
Sexual Abuse
Sexual Abuse is when a child or young person is told, asked or forced to take part in sexual activity. The ways in which a young person can be sexually abused may involve physical contact, including assault by penetration, rape, oral sex; making them do sexual things either to themselves or with other people; kissing, touching and rubbing outside of clothing.
Involving them in the making of films or taking photos that involve sexual activity; making them watch sexual behaviour (non-contact activities); whether or not the child is aware of what is happening.
It is crucial to understand that sexual abuse perpetrators are not only adult males. Women can also commit acts of sexual abuse, as can other children.
All staff must be aware that penetrative sex where one of the partners is under the age of 16 is illegal. Although prosecution of similar age, consenting partners is not usual, but immediate advice should be taken from the DDCS Safeguarding Lead AND local team. However, where a child is under the age of 13 it is classified as rape under Section 5 Sexual Offences Act 2003.
See Sexual Offences Act 2003 (legislation.gov.uk)
Neglect
Neglect is when a child or young person is not properly looked after. This could damage their health or wellbeing. A child's basic needs include food and shelter; safety within the home; proper clothing; good cleanliness; warmth; receiving necessary medical treatment; protection from physical and emotional harm or danger.
Potential Risk of Harm to an Unborn Child
Neglect may occur during pregnancy due to maternal substance misuse, mental ill health or learning difficulties. Domestic abuse and violence towards a carer may also cause to neglect the needs of an unborn child.
In any circumstances when staff are able to anticipate the likelihood of significant harm to an expected baby, concerns should be addressed as early as possible before the birth to provide safe care and support if possible.
See: https://learning.nspcc.org.uk/child-abuse-and-neglect/neglect
Child Sexual Exploitation (CSE)
Sexual exploitation of children and young people under 18 involves exploitative situations, contexts and relationships where a young person or a third person receives something (e.g. food, accommodation, drugs, alcohol, gifts, cigarettes, affections or money) as a result of them performing and/or another or others performing on them, sexual activities.
CSE can occur through the use of technology without the child’s immediate recognition; for example, being persuaded to post sexual images on the internet/mobile phones without immediate payment or gain. In all cases those exploiting the child/young person have power over them by virtue of their age, gender, intellect physical strength and/or economic or other resources
Violence, coercion and intimidations are common, involvement in exploitative relationships being characterised in the main by the child’s or young person’s limited availability of choice resulting from their social and economic and/or emotional availability (DH, 2009).
CSE often starts at the age of 12-13 and victims can be girls or boys regardless their ethnicity, religion or cultural/social background.
Especially Vulnerable Groups:
■ Looked After Children
■ Children Leaving Care
■ Children Missing from school home or care
■ Children with learning difficulties
The potential indicators of risk of being sexually exploited are:
■ Missing from home or care
■ Physical injuries
■ Drug or alcohol misuse
■ Involvement in offending
■ Repeat sexually transmitted infections, pregnancy and terminations
■ Absent from school
■ Change in physical appearance
■ Evidence of sexual bullying and/or vulnerability through the internet and/or social networking sites
■ Estranged from their family
■ Receipt of gifts from unknown sources
■ Recruiting others into exploitative situations
■ Poor mental health
■ Self-harm
■ Thoughts of suicidal ideation or attempts at suicide
DDCS Staff must always be mindful of the above when seeing and/or assessing children and their family in the course of their delivery activities and act accordingly.
Staff must remember that CSE is sexual abuse, and every possible action must be taken to safeguard the child or young person first including referring on to appropriate agencies.
All CSE cases or probable CSE must be referred to the Local Authority, following the Local Authority’s threshold, by using the appropriate referral form. See London Safeguarding Children Partnership – CSE guidance or HM Gov– Report Child Abuse
This referral must be made regardless of any other immediate actions have been taken to reduce harm to a child or a young person.
Online Safety (Information & Communication Technology)
Although communication via internet has many positive outcomes however, it poses huge amount of risk of abuse to the children. Children are at risk of physical, sexual and emotional abuse; radicalisation; and bullying via mobile telephones or online (internet) with verbal and visual messages.
Bullying is the most common form of behaviour that children and young people complain about online abuse. DDCS staff must raise this awareness amongst the children, parents and carers.
The impact on a child of internet-based sexual abuse is similar to that for all sexually abused children However, it has an additional dimension of there being a visual record of the abuse. Internet based sexual abuse of a child constitutes significant harm through sexual and emotional abuse.
Concept of significant harm, as a situation where a child is suffering; or is likely to suffer a degree of physical; sexual; and/or emotional harm, through abuse or neglect; which is so harmful that there needs to be compulsory intervention by child protection agencies into the life of the child and their family.
All DDCS Staff working with children, adults and families should be alert to the possibility that:
■ A child may already have been/is being, abused and the images distributed on the internet or by mobile telephone.
■ An adult or older child may be grooming a child for sexual abuse, including for involvement in making abusive images. This process can involve the child being shown abusive images
■ An adult or older child may be viewing and downloading child sexual abuse images.
Where the concerns involve a particular child/ren, professionals considering/ making a referral to local authority children's social care should do so in line with the reporting guidelines below.
All staff should be aware that the child may not want to acknowledge their involvement or admit its abusive nature, and may resist efforts to offer protection. This should not be a deterrent and the DDCS Safeguarding advisor and or local safeguarding team should be contacted for support and advice.
All provider staff must always follow the organisations email and internet policies.
Fabricated Illness
For those children who have had illness fabricated or induced are likely to require co-ordinated help from all agencies. Joint working is essential to safeguard the child and where necessary take action within the criminal justice system thus all professionals must be alert to potential indicators of abuse:
■ Be alert to the risk of harm which individual abusers or potential abusers may pose to children in whom illness is being fabricated or induced.
■ Share and help analyse information so that an informed assessment can be made of the child’s needs and circumstances.
■ Contribute to whatever actions (including the cessation of unnecessary medical intervention) and services to safeguard and promote the child’s welfare.
■ Assist in providing relevant evidence in any criminal or civil proceedings, should this course of action be deemed necessary.
Identifying Fabricated or Induced Illness is neither a swift nor easy process. Identifying the carer’s patterns of behaviour will take a multi-agency approach, expertise and observation. There are three main ways a carer fabricates or induces illness in a child, they are not mutually inclusive but include:
■ Fabrication of signs and symptoms, including giving a grossly exaggerated or false past medical history
■ Falsification of test results and records, this includes altering charts and records and substituting specimens of body fluids
■ Induction of illness by a variety of means
Concerns may be raised when it is considered that the health or development of a child is likely to be significantly impaired or further impaired by a parent or care giver who has fabricated or induced illness these concerns may arise when one or the more factors are encountered:
■ Reported symptoms and signs found on examination are not fully explained by any medical condition from which the child is suffering
■ Physical examination and results of medical investigations do not explain the reported symptoms and signs or there is an inexplicably poor response to prescribed medication and other treatment
■ New symptoms are reported on resolution of previous ones
■ Reported symptoms and found signs are not seen in the absence of the carer
■ Over time the child is repeatedly presented with a range of signs and symptoms
■ The child’s normal daily life activities are being curtailed beyond that which might be expected for any medical disorder from which the child is known to suffer.
There may be several explanations for these circumstances, and each requires careful consideration and review.
A developmental history and developmental assessment should be undertaken by appropriately trained and qualified specialist clinical staff such as Community Paediatricians, or Safeguarding specialist Nursing or other appropriate staffing groups.
Consultation with professional peers, the DDCS Safeguarding Lead, Local safeguarding system named or designated professionals or colleagues in other agencies will be an important part of the process of making sense of the underlying reason for the signs and symptoms.
This is not currently an area of activity that DDCS is conceivably involved in, but it is essential that DDCS staff are aware of the wider system response in support of the Children’s safeguarding agenda.
The characteristics of fabricated or induced illness are that there is a lack of the usual corroboration of findings with signs and symptoms, or, in circumstances of proven organic illness, lack of usual response to proven effective treatments. It is this puzzling discrepancy that normally alerts the clinician to possible harm being suffered by the child.
The following features can be associated with this form of abuse, though none is indicative in itself:
■ The child’s medical, especially hospital treatment begins at an early stage of their ‘illness’.
■ They attend for treatment at various hospitals and other healthcare settings in different geographical areas.
■ They may develop a feeding disorder as a result of unpleasant feeding interactions.
■ Non-organic failure to thrive.
■ The child develops an abnormal attitude to his/her own health.
■ Poor school attendance and under achievement.
■ Incongruity between the seriousness of the story and the actions of the parents.
■ The child may already have suffered other forms of abuse.
■ Erroneous or misleading information provided by the carer.
■ History of unexplained death, illness, or multiple surgery in parents and/or siblings.
■ Carer history of childhood abuse, false allegations of physical or sexual assault, self-harm or psychiatric disorder (especially personality disorder or psychotic illness).
■ Carer over-involvement in medical tests, taking temperatures or measuring bodily fluids.
■ Carers observed to be intensely involved with the child, e.g. not allowing anyone else to undertake their child’s care.
■ Carers may appear unusually concerned about the results of investigations that may indicate physical illness in the child, although conversely, they may not appear at all concerned.
■ Health professionals who have concerns or a suspicion that fabricated or induced Illness is being presented must consult with their Named/Designated Doctor and/or Named/Designated Nurse.
■ There may be a number of explanations for these circumstances. Careful consideration and review of information should be undertaken in consultation with peers and colleagues both within their own and other agencies, including the Designated Doctor / Designated Nurse Safeguarding Children.
■ A medical opinion should be sought through a Consultant Paediatrician. Symptoms and signs require careful evaluation alongside results of tests and observations.
■ A chronology of health involvement, including access to all health services should be prepared to provide comprehensive information.
■ Any relevant information relating to the parents or siblings’ medical history should be shared appropriately with other health professionals. Practitioners should seek advice about sharing this information without consent, but lack of consent must not hinder the process. When no explanation can be found for the condition this should be recorded in the child’s records, and the Paediatrician informs the carers that there is no explanation and records the carer’s response.
■ A future plan as to further tests, investigations or assessments, which maybe in a specialist setting, should be shared with the carers. Carers whilst being kept informed should “at no time have the concerns about the reasons for the child’s signs and symptoms shared with them, if information would jeopardise the child’s safety”.
■ Health records should be kept secure to prevent tampering and all entries legible, signed and dated. All records and referral letters should be completed and maintained in chronological order. If a health professional considers their concerns are not being responded to appropriately, the concerns should be discussed with the Designated Doctor/Nurse Safeguarding Children.
■ Following medical investigation, consultation and review being undertaken in consultation with the Named or Designated Doctor Safeguarding Children, and there is a possible explanation that the child’s signs and symptoms may be fabricated or induced illness, a referral to Children’s Social care should be made.
■ In general, a referral would normally be undertaken with the permission of the parent/carers however this should only be done where informing the parent/carer will not place the child at increased risk of significant harm.
■ Children’s Social Care will have lead responsibility for actions to safeguard the child: the Paediatric Consultant will continue to hold the responsibility for the child’s health and decisions pertaining to it. All three agencies should work closely together making joint decisions, especially about sharing information with the carers.
■ All information and information sharing should be documented clearly. Promoting children’s well-being and safeguarding them from harm depends crucially on effective information sharing, collaboration and understanding between agencies and professionals. In cases where there is concern that illnesses are being fabricated/induced, there may be a difference of opinion about how to best safeguard a child’s welfare.
-
All Staff have a key role to play in actively promoting the health and wellbeing of children. Section 11 of the Children Act 2004 places a duty on all providers of NHS services in so much that they have regard to the need to safeguard and promote the welfare of children.
All health professionals who work with children and families should be able to:
Understand the risk factors and recognise children in need of support and/or safeguarding
■ Recognise the needs of parents who may need extra help in bringing up their children and know where to refer for help
■ Recognise the risks of abuse to an unborn child
■ Contribute to enquiries from other professionals about children and their family or carers
■ Liaise closely with other agencies, including other health professionals
■ Assess the needs of children and the capacity of parents/carers to meet their children’s needs, including the needs of children who display sexually harmful behaviour
■ Plan and respond to the needs of children and their families, particularly those who are vulnerable
■ Contribute to child protection conferences, family group conferences and strategy discussions
■ Contribute to planning support for children at risk of significant harm, e.g., children living in households with domestic violence or parental substance misuse
■ Help ensure that children who have been abused and parents under stress (e.g., those who have mental health problems) have access to services to support them
■ Play an active part, through the child protection plan, in safeguarding children from significant harm
■ As part of generally safeguarding children and young people, providing ongoing promotional and preventative support, through proactive work with children families and expectant parents
■ Contribute to serious case reviews (SCRs) and their implementation
-
Evidence suggests that Children and their families who receive coordinated early help are less likely to develop difficulties that require intervention through a statutory assessment under the Children Act 1989.
Children, young people and families experience a range of needs at different times in their lives. The common assessment framework (CAF), proposed by Every Child Matters, and Local Authorities’ thresholds are a way of working out what extra support a child may need and how best to provide it. See London Safeguarding Children Partnership’s resource on Referral and Assessment for additional help. Confidentiality and Data protection must be taken seriously while sharing information and making referrals. However, this should not be a barrier to safeguard a child or a young person.
-
Where there are significant concerns about the safety of a child or children, professionals should contact 999 or Local Council Social Care teams.
Any discussion, referral and advice must be recorded appropriately in clinical records.
When making a referral staffs must ensure to:
■ inform the social services whether just requesting advice or making a referral.
■ Confirm that speaking to an appropriate person who is in a position to take the referral, record their name and position.
■ must have the appropriate facts to hand in order to make a clear referral statement.
Referrals are made in accordance with the instructions on the referral form by first telephoning Children’s Social Care with all relevant details before emailing the completed form through to them.
Completed referral forms should only be sent to and from secure email.
If there is an alleged crime of abuse towards a child, staff may need to refer directly to the police (and/or social care).
-
Section 47 of the Children Act 1989 gives the local authority a statutory duty to make enquiries when it has reasonable cause that a child is suffering or likely to suffer significant harm. Section 47 therefore empowers local authorities to call upon other professionals and agencies to assist them.
When carrying out Section 47 enquiries the local authority has a statutory duty to obtain access to the child’s health information and therefore this duty is not subject to permission by those with parental responsibility.
Staff should act promptly to support local authority when section 47 requests are received by providing accurate up to date information.
Section 17 of the Children Act 1989 places a general duty with social care to safeguard and promote the welfare of children in their area who are in need, as with Section 47 they can call upon other professionals and agencies to assist them.
The assessment uses a systematic approach to assessing a child in need.
Staff must provide specific information to the local authority as quickly as possible when information is requested under section 17.
-
There are 4 types of child protection conferences:
■ Initial conferences
■ Pre-birth conferences
■ Transfer in conferences
■ Review conferences
All child protection conferences should include not only the child subject of the specific concerns but must also include consideration of the needs of all other children in the household.
An initial child protection conference must be convened when the outcome of the Section 47 enquiry confirms that the child is suffering, or is likely to suffer, significant harm. The local authority children's social care manager is responsible for making the decision on the completion of the Section 47 enquiry.
Every review should consider explicitly whether the child is suffering, or is likely to suffer, significant harm and hence continues to require safeguarding from harm through adherence to a formal child protection plan. If the child is considered to be suffering significant harm, the local authority should consider whether to initiate family court proceedings. If not, then the child should no longer be the subject of a child protection plan and the conference should consider what continuing support services may benefit the child and family and make recommendations accordingly.
If DDCS staff receives a request to attend a case conference, then the conference should be attended by an appropriate health professional supported by the DDCS Safeguarding Lead senior team member/line manager if necessary. A report should be prepared and submitted within the time line given by the local authority. The attendee must have relevant information and history of the child and family and also have adequate clinical/professional knowledge and skill to represent the child and professionally challenge any disagreement. If there is disagreement about the decision during the conference between agencies, the conflict resolution procedures should be applied.
In a situation where an DDCS staff member or contractor thinks there are other Health Professionals more appropriate to attend the Case Conference (e.g. the child is under the care of another clinical service area) they should discuss this with the DDCS Safeguarding Lead and if agreed ensure that they forward all information to the relevant Health Professional without any delay.
This is to ensure that the attending Health Professional has got more current, relevant and greater information about the child and the family. The DDCS member must give support to the attending Health Professional to write a report and attend Case Conferences if requested to do so.
In a case where there is a disagreement around who attends the Case Conference this should be immediately escalated to the DDCS Safeguarding Lead and DDCS Director. All staff must be aware that any confusion and escalation must not be a barrier or reason not to attend a Case Conference.
-
If a child has been put on child protection plan or child in need plan, appropriate health professionals involved in the clinical or social care of the child or young person must take applicable actions and support the child or children and family to meet their needs.
They must continue to work closely with the child/ren, family and other partners to ensure all allocated action plans are met to keep the child/children or young person safe.
They must remain vigilant and carry out continuous risk assessment to ensure safety.
As soon as an universal health professional (such as a school nurse and health visitor) is informed that a child is either on child protection plan or a child in need, appropriate flag must be activated on relevant systems – such as System One or a GP System of Choice via a Primary Care Network or similar access mode - by them. DDCS staff will not ordinarily have access to this information, and not ordinarily be leading on data updates of this nature but may become aware of individual status due to involvement in services or care delivery.
De-escalating the flag remains the responsibility of the lead universal health professionals. Unless any other health professional becomes aware of this before a school nurse or a health visitor then it becomes other health professional’s responsibility to pass on this information or if they have appropriate access to core clinical or social care records to ensure this is updated by them.
-
Concern or disagreement may arise over another professional’s decisions, actions or lack of actions, in relation to a referral, an assessment or an enquiry. Overwhelmingly these will involve the lead agencies and universal healthcare providers from acute or community settings, and the role of DDCS is likely to be that of providing supportive input rather than initiating and or convening its own multiagency processes or initiating and coordinating actions such as Section 47 enquiries where legislative and guidance points to other elements of the multi-agency environment for the key responsibilities.
It is important to note and adhere to the following principles that inform the wider system responses and the issues that may occur in the multi-agency environment: where DDCS may have a role:
■ The safety of individual child/ren and focus on child/ren are the paramount considerations in any professional disagreement and any unresolved issues should be escalated.
■ Avoid professional disputes that put children at risk or obscure the focus of the child
■ Resolve difficulties (within and) between agencies quickly and openly
■ Identify problem areas in working together where there is a lack of clarity and to promote resolution via amendment to protocols and procedures.
Disagreement may also arise regarding response to a referral made to Social Care, e.g:
■ whether eligibility criteria are met
■ whether concerns justify a Section 47 enquiry
■ whether to convene an initial case conference - NB invitation to participate in one should never be a source of disagreement – if an invitation is offered it must be accepted by DDCS.
Dissent can also arise regarding decisions made at case conferences or subsequently regarding implementation of a Child Protection Plan. If a local resolution cannot be agreed, then this must be escalated to more senior staff with wider experience of safeguarding concerns. In the context of DDCS, this is unlikely to arise as the flat structure of the organisation and direct involvement in safeguarding discussions of the DDCS Safeguarding Lead will provide appropriate seniority and experience for DDCS to engage with any escalation of concerns that may occur.
-
DDCS will make every effort to ensure safe recruitment of all staff. However, in an unfortunate event where there is an accusation of abuse against an DDCS Employee or subcontractor the Director and the Safeguarding Lead must be notified. The DDCS employment processes – including ‘Disciplinary Procedure’ and any contractual requirements flowing from commissioned works must be followed.
Crucially, appropriate referrals to Children’s Social Care will be enacted within the timeframes stipulated and Local Authority & Designated Officer will be informed.
This can apply when a member of staff has:
■ Behaved in a way that has or may have harmed a child
■ Possibly committed a criminal offence against or related to a child
■ Behaved towards a child in a way which indicates he/she is unsuitable to work with a child.
If the Employee or subcontractor has allegedly committed a criminal offence:
■ The Director and Safeguarding Lead must be contacted without delay and if necessary the local Police must be contacted.
■ If the allegation is against the Director and Safeguarding Lead, then the local safeguarding system leads ( Assistant Director and Safeguarding Team) must be notified.
■ Where any concerns regarding an employee’s suitability to work with children or vulnerable adults is identified, the employer must refer the case to the DBS and any relevant professional body.
DDCS will work together with local authority children's social care and/or other partners to protect the child/ren and family. DDCS must consider the impact on the child concerned and provide support as appropriate. Liaison between the agencies should take place to ensure that the child's needs are addressed.
If DDCS staff or subcontractors becomes aware of any information regarding another member of DDCS staff or contractors which identifies that a child/ren may be at risk of harm or has been harmed (including the member of staff’s own child/children), they must immediately report this information to their line manager and make referral to the social services/police if necessary.
The information must also be shared with the DDCS Safeguarding Advisor for who will be responsible for sharing appropriately within DDCS as well as notifying Social Care and LADO and or Police as appropriate. As with all investigations, a police / criminal line of enquiry will take precedence above all others.
-
All staff that work with children should ensure that they have the skills and knowledge as set out in ‘Intercollegiate Document’ as described in section 2 above.
Safeguarding Children awareness must be covered within the DDCS induction for all new staff, and sub-contractors and new staff should also receive additional local introductory training in safeguarding children from their supervisor/ line manager. At Induction Training, all DDCS staff must be informed of the Safeguarding Children Policy and Guidelines.
All DDCS staff must receive training and regular updates at the appropriate level for their role. It is mandatory for all staff working with children, families, and parents/carers of children to attend training updates.
All staff must ensure that they are aware of their responsibility to attend safeguarding children training in accordance with local training Policy and familiarise themselves with the DDCS training arrangements.
Any member of staff unsure of their training needs should contact the DDCS Safeguarding Lead to discuss their requirements.
A note on supervision
Child Protection/Safeguarding Children supervision is mandatory for all health professionals working with children and their families. Currently DDCS staff do not deliver work of the nature, and the following is a suggested text should DDCS ever require that supervision structures are established to support safeguarding works not currently delivered.
In general, a proactive approach to supervision is required to ensure that all staff are supported and continue to develop their skills and knowledge in recognising and acting on concerns regarding the safeguarding of children and responding to the needs of vulnerable children.
■ Operational Service Delivery Leads must ensure that protected time is available to enable staff to receive supervision in accordance with the guidelines.
■ Child protection/safeguarding children support, and supervision will be provided in addition to clinical supervision and management supervision.
■ The DDCS Safeguarding Lead can provide supervision – but not clinical supervision - to encourage reflection, development and support for DDCS staff.
Supervision arrangements will be reviewed in line with the consideration of contracted and commissioned services as set out above in the Introduction and section 5 above.
-
HM Gov 2021
Children Act 1989. London: HMSO
Children Act 2004. London: HMSO
Common Core of Skills and Knowledge for the Children’s Workforce. London. HM Government 2005.
CQC Essential: Standards of Quality and Safety 2010
Jago, S. & Pearce, J.: Gathering evidence of the sexual exploitation of children and young people: a scoping exercise Luton: University of Bedfordshire 2008.
Intercollegiate Document Safeguarding Children Roles and Competencies for Health Care Staff RCN 2019
Safeguarding Children & Young people from Sexual Exploitation DH 2009
Sexual Offence AcT 2003
Working Together to Safeguard Children a guide to inter-agency working to safeguard and promote the welfare of children. HM Government (2015)
London Safeguarding Children’s Partnership
Acknowledgements
Provide Safeguarding Policy suite
Social Care Institute for Excellence
HMG Safeguarding Children Policies, procedures and guidance
Policy updates
The Director and Programme Associates are responsible for updating this policy. This policy will be adapted to reflect changes in national legislation and statutory guidance and delivery in accordance with local safeguarding and other relevant partnership arrangements.
This statement is approved by the Director, Dan Devitt.
Questions, comments and requests regarding this policy are welcomed and should be addressed to info@ddconsultancyservices.com.
Version 1.0, adopted 18th November 2025